If AI Can Recreate a Movie Star, Is It Ready for Your Health Record?
Visual AI progress is fascinating. But it does not automatically signal that AI is ready to operate inside complex health systems at scale.

Over the past week, headlines described a new AI video generator capable of producing highly realistic scenes featuring well-known actors. The reaction in parts of the film industry was immediate. Excitement. Concern. A sense that something fundamental had shifted.
It is impressive technology.
But I have already heard a version of the same sentence several times:
“If AI can do that, imagine what it can do in healthcare.”
That leap is understandable. It is also flawed.
Let’s unpack why, carefully.
The seduction of visible progress
Visual AI progress is easy to see. You watch a clip. It looks real. The system appears intelligent.
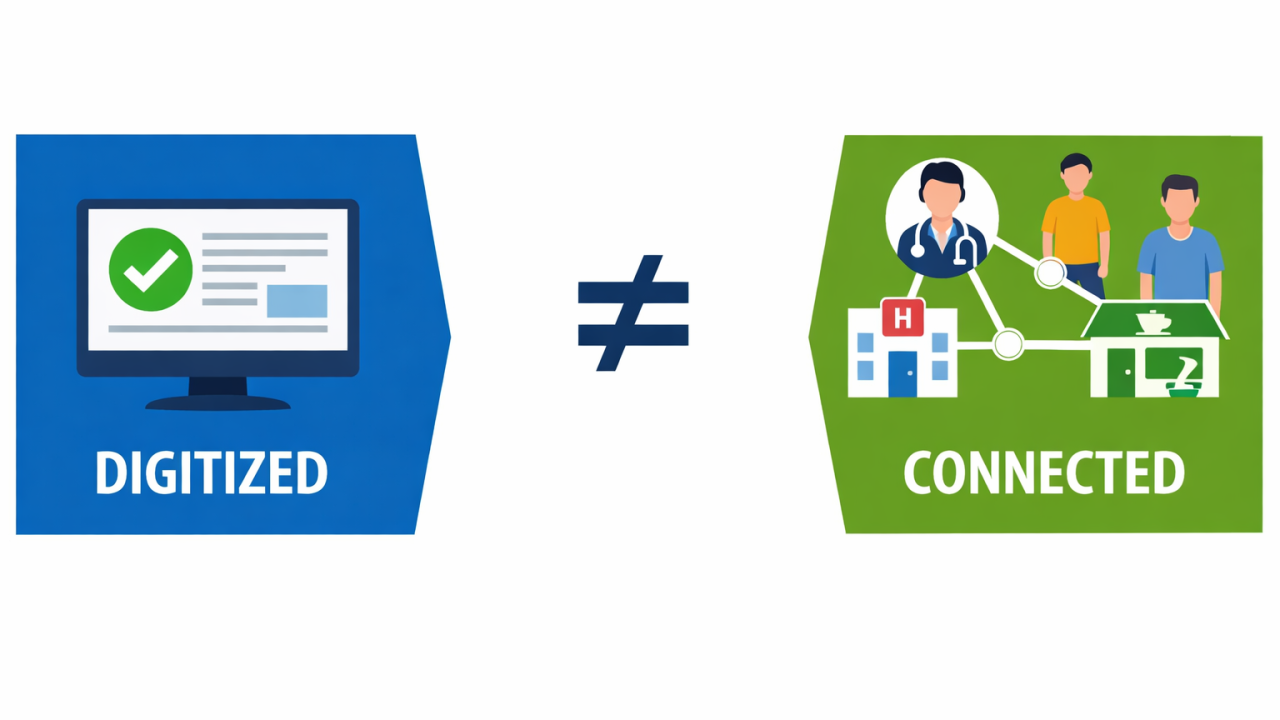
Healthcare AI progress is harder to see. It happens in validation studies, regulatory submissions, workflow pilots, and governance reviews. It is slower. It is less cinematic. It is also more consequential.
The mistake is assuming that visible technical sophistication equals readiness for clinical responsibility.
It does not.
Entertainment optimizes for realism. Healthcare must optimize for safety.
A video generator is judged by whether it produces something that looks convincing. If it improves through iteration and scale, that is viewed as progress.
Healthcare AI is judged differently. It must demonstrate clinical validity, safety, equity, and reliability in real-world conditions. It must withstand scrutiny from regulators, clinicians, patients, and legal systems.
The World Health Organization has explicitly stated that AI in health requires strong governance, transparency, and human oversight across its lifecycle. Innovation alone is insufficient.
A compelling output is not the same as a safe clinical recommendation.
Regulation is not friction. It is protection.
In healthcare, AI systems that inform diagnosis or treatment may be regulated as medical devices.
In the United States, the Food and Drug Administration has issued a formal action plan for AI and machine learning based medical devices. It addresses pre market review, post market monitoring, and change management for adaptive systems.
In Canada, Health Canada has published guidance aligned with Good Machine Learning Practice for medical device development.
These frameworks exist because error in healthcare is not an inconvenience. It can cause harm.
Entertainment can iterate in public. Healthcare must validate before scale.
Accuracy in a dataset is not readiness in a system
A model can perform well in retrospective testing and still fail ethically or operationally in practice.
A widely cited study published in Science showed that a health management algorithm used in the United States underestimated the needs of Black patients because it used healthcare spending as a proxy for illness burden. The issue was not a technical malfunction. It was a structural design choice that embedded bias.
Healthcare AI must therefore be tested not only for accuracy but for fairness, population performance, and unintended consequences.
That requires time, oversight, and accountability.
No visual breakthrough changes that reality.
Healthcare readiness is a system question, not a model question
Even when an AI model performs well, there are additional barriers:
• Integration into electronic health records
• Workflow redesign
• Clinician training
• Data quality controls
• Cybersecurity safeguards
• Legal clarity on accountability
Technology capability does not automatically resolve these.
In digital health work, I have seen strong technical solutions stall because the surrounding system was not prepared. Readiness is as much about governance and culture as it is about algorithms.
The deeper misconception
The narrative emerging from entertainment headlines is simple:
AI is accelerating. Therefore, all sectors should accelerate equally.
Healthcare cannot operate that way.
The tolerance for risk is different. The burden of proof is higher. The ethical stakes are greater.
This does not mean healthcare AI is not advancing. It is. There are approved systems in imaging, cardiology, pathology, and operational analytics that are delivering value today.
But those systems reached deployment through evidence, regulation, and structured oversight.
That path will always look slower than viral breakthroughs in media.
And it should.
A leadership reflection
The real leadership question is not whether AI is powerful. That is already clear.
The question is whether we are distinguishing between technological possibility and clinical responsibility.
In healthcare, speed is not the primary metric.
Safety, trust, equity, and governance are.
Visual AI progress is fascinating. It may reshape creative industries.
But it does not automatically signal that AI is ready to operate inside complex health systems at scale.
Healthcare deserves disciplined implementation, not technological optimism.
References
World Health Organization. Ethics and Governance of Artificial Intelligence for Health. 2023. https://www.who.int/publications/i/item/9789240029200
U.S. Food and Drug Administration. Artificial Intelligence and Machine Learning Based Software as a Medical Device Action Plan. 2021. https://www.fda.gov/media/145022/download
Health Canada. Good Machine Learning Practice for Medical Device Development. 2023. https://www.canada.ca/en/health-canada/services/drugs-health-products/medical-devices/activities/guidances.html
Obermeyer Z, Powers B, Vogeli C, Mullainathan S. Dissecting racial bias in an algorithm used to manage the health of populations. Science. 2019. https://www.science.org/doi/10.1126/science.aax2342
Latest Insights